Sumio Makino (Advisor,JIRA)  |
1.Sequel to "Development of Nuclear Medicine Equipment-1" (Mr. Sumio Makino)
Japanese people's experience with "radioactivity" originated from the first sad incident. It originated from the atomic bombs that were dropped over the cities of Hiroshima and Nagasaki, killing instantly hundreds of thousands of people in August 1945.
In the History column of "JIRA Bulletin No. 10," I wrote about the origin of radiation technology in Japan. In that article, I referred to the development of radiation meters.
During the very period of the development of the device, the second incident occurred in 1954. The U.S. conducted the "H-bomb test" at the Bikini Atoll. The radioactive ash fallout contaminated a tuna fishing boat, "the Fukuryumaru No. 5," which was headquartered at Yaizu Port, Shizuoka Prefecture. A fisherman, Mr. Kuboyama, died from the acute radiation exposure.
The Second World War devastated Japan and Japanese people. In 1950, however, the "Korean War" broke out, resulting in the "special procurements" of industrial products, thus revitalizing the Japanese economy and industry. In keeping pace with this, the academic and medical societies were reborn from the postwar devastation.
In 1947 and 1948, the academic societies started at last the study in foreign countries. The late Hisao Yamashita MD (Keio University) and the late Hirotake Kakehi MD (the University of Tokyo, lecturer) went to radiological research institutes in the U.S. and Canada for study. They told us the results of overseas study and gave us guidance.
2. The first meeting in the postwar period: "R1 Measuring-Method Study Session" held at the University of Tokyo:
First of all, they established "Tokyo University R1 laboratory." Soon after the establishment, they held a 10-day training course for RI measuring method. The venue was the underground laboratory, where young researchers gathered. The course was guided by the late professor Masanori Nakaizumi and the late lecturer Kakehi, both from Tokyo University, School of Medicine, Radiology Department. Several manufacturers (such as Toshiba, Shimadzu, Kobe Kogyo) provided the RI meters. Then, the writer represented Toshiba and took five sets of the centesimal counters there (Fig. -1).
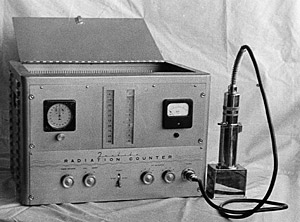 |
| Fig. 1 the centesimal counters |
The radiation detection tubes were all Geiger-Mueller tubes. All the counters used vacuum tubes. The centesimal counter used about 20 vacuum tubes. As a result, the chassis of counter was heated like an electric heater. The heat damaged the delicate resistors of control circuit. When we continued measurement for several hours at the course, correct measurement was impossible. The writer readjusted the counters at night every day during the course period so that the counters might be available for measurement the next day. All the counters of other manufacturers failed to function. The writer wants to record this happening as an episode of the postwar history.
3. Direct Medical Application of RI Attempted
(1) Trial production of Strontium 90 applicator for ophthalmology
Sr90 was a beta ray emitting RI with a long half-life. Professor Masanori Nakaizumi, the University of Tokyo, recommended us to produce a beta ray radiotherapy equipment for ophthalmology. We attempted to insert Sr90 into the tip of the applicator that looked like a large fountain pen.
At that time, we had no facilities like a hot laboratory. We handled Sr90 solution and everywhere was contaminated with adhesion of solution. We understood how difficult it was to handle radioactive substances, and failed in completion of a product.
(2)Development of the teletherapy equipment with a mass of Co60
This is recorded in detail in the History column of "JIRA Bulletin 2001, 1." The title is "Development of Radiological Equipment in the Postwar Japan-15."
(3)Progress and expanding application of radiation meters
The detector for radiation meter used immediately after the war was an ion chamber. Later, it progressed into the Geiger-counter tube.
The ion chamber measures the gas ion current generated by radiation. The gas is sealed in the chamber. A very small current is subjected to direct-current amplification, and converted to a reading of radiation dose. The demerit was that its sensitivity was lower than that of meters that were invented later.
A Geiger Muller Counter is a vacuum tube in which the ion gas and the quenching gas are sealed. The structure and material of the window at the tip were different, depending on measurement of beta ray or gamma ray. An output is pulses proportional to radiation dose. The output is measured with a rate meter or a counter, thus to measure radiation dose.
The meters available until that time were used mainly for physics and physical science measurement.
Around 1960, the scintillation crystal appeared as the solid-state detector. Compared with the previous detectors, the solid-state detector was more sensitive and easier to use, being employed for many radiation meters.
Initially, the size of crystal was 1 to 2 inches. The size increased to 4, and then to 12 inches. The large crystal was used for medical application, such as the thyroid function test.
4. Origin of RI medical imaging
The first medical application of scintillation counter was the "scintiscanner."
 |
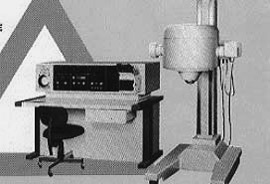
| Fig. 2 the first scintiscanner made in Japan |
Lecturer Hirotake Kakehi, the University of Tokyo, School of Medicine, Radiology Department became professor at Chiba University, Radiology Department. Soon after that, the scintiscanner of the U.S. Tracer Lab. was installed there and medical use was started. Then, the professor taught the writer the essence of medical application of the scintiscanner, a new diagnostic equipment. In the U.S., he underwent RI nuclear medicine training. After returning to Japan, he opened the department of nuclear medicine at Chiba University, School of Medicine. He imported a scintiscanner from the U.S. as mentioned above and endeavored to establish nuclear medicine.
We followed his guidance, investigated the imported scintiscanner, and started the design work to produce the equipment in Japan.
Although the crystal used then was as small as 2 inches, we succeeded in making a prototype and offered it to Professor Kakehi for his trial use.
Fig. 2 shows the scintiscanner with a 2-inch crystal, which was made for the first time in 1960 in Japan.
Subsequently, the scanner with a 4-inch crystal became popular.
At the early stage of development, there were many difficulties in producing the scanner. The longitudinal and lateral scanning was not uniform. Especially, the interval in the longitudinal scanning was not uniform.
While scintiscanners were in use, Professor Anger and others at University of Chicago developed and announced a scintillation camera. The camera became suddenly the main equipment for nuclear medicine imaging.
Development of Radiological Equipment in the Postwar Japan-No. 2
Development of Nuclear Medicine Equipment-2
Shigeyasu Kurihara(JIRA, former chairman) |
1. Sequel to "Development of Nuclear Medicine Equipment-1" (Mr. Sumio Makino)I was told to write about the scintiscanner. It is 40 years ago that I was involved in the task. I have no documents at hands. Please forgive me, if my memory is not correct.
In the preceding article, Mr. Makino mentioned the scanner made in Japan for the first time in 1960. Then, the size of detector increased to 3, 4 and 5 inches. The scanner with two detectors facing each other was also developed. On the other hand, several types of recorders were developed, including the discharge recording paper, the photo-recording, color recording (several variations), and multi-dot (Japanese invention). The image quality was improved by the contrast enhancement, simultaneous multi-nuclide scan, tomographic scan, equi-sensitivity scan, etc.
2. Before Commercial Production of Anger Type Scinticamera
Until the scinticamera was imported in 1967, the scanner had been the main equipment for R1 diagnostic imaging. After the nuclide of Technetium 99m became available in Japan, the demand for the scinticamera went up sharply in the Japanese market. The Anger type camera was patent-licensed in the U.S. exclusively by the U.S. Nuclear Chicago Corp. (N.C. Corp.). After Mr. Anger announced the principle of camera in 1958, the camera attracted attention as the next-generation RI imaging equipment capable of dynamic study. Other types were developed in the U.S., such as the I.I. camera of Ter-Pogossian type, the autofluoroscope by Mr. Bender and Mr. Blau, The spark chamber type was also announced. At that time, Toshiba Corp. searched for the possibilities other than Anger type and developed several prototypes, including the solar slit camera (see the paper B7-6 for the 9th RI conference in 1969) and the multi-stage image-tube type camera (for the 14th RSNA in June 1967, Seattle) that was developed jointly by Dr. Iio, Ueda Department of Internal Medicine, the University of Tokyo.

3. Participation in the North American Nuclear Medicine Community, and Subsequent Inspection Tour
After attending the conference in Seattle in June 1967, the writer and some Japanese doctors joined the inspection tour to the prestigious laboratories, hospitals and manufacturers related to nuclear medicine. We visited Mayo Clinic, Abbott Lab., N.C. Corp. (now, Siemens), Chicago Univ. Washington Univ. (Ter-Pogossian camera), Oak Ridge National Laboratory, Roswell Park Cancer Institute (Bender/Blau camera), and Harshaw Chemical (structure of scintillation crystal). We investigated the directivity of development of U.S. nuclear medicine.
As a conclusion at this time, we thought that radiopharmaceuticals would be developed and imported to Japan and that the clinical application would be expanded rapidly. In order to use the radiopharmaceuticals, the Anger type camera was most suitable. It was necessary to produce the camera in Japan as soon as possible. On our way home, we stopped at San Francisco, visiting Donner Lab., Berkley, and interviewing Mr. Anger. We negotiated that he would grant us the patent license, but we were told that he granted all of the license to N.C. Corp. and that the patent was applicable in the U.S.
4. Domestic Production of Scinticamera (Gamma camera)
In 1967 and 1968, about 20 sets of the N. C. Corp. scinticameras were imported and installed at the Japanese leading facilities of nuclear medicine (being distributed by Shimadzu). The request for domestic production of the camera was strong. The exchange rate was 360 yen per dollar, and foreign currency was scarce. National hospitals had financial difficulty for imports. A special development budget of the then Science and Technology Agency was acquired by National Kohnodai Hospital for the 1968 fiscal year. Toshiba Corp. promised to complete the development project within one year. The writer and colleagues explained to the General Manager of Division how we planned to complete this project. In order to keep the very tight deadline, we were forced to cannibalize even some systems that had failed until then. We experienced cold-sweat nightmares.
We cannibalized the above-mentioned multi-image tube equipment and reused the crystal and collimator. Our experience was not useless. The principle of Anger type was already announced in the academic journal in 1958. Our basic design had been completed. A medical physicist in Tokyo was kind enough to show us how to use the imported product, and to tell us the characteristics and data.
During the 10 months after the receipt of order, we proceeded with design, part procurement, and sub-assembly of components. We built a breadboard for the imaging experiment. In August, we had a bright outlook for production. The project proceeded at a stretch to the final stage of production. We delivered the camera to the hospital in March 1969 just on time for the fiscal 1968 budget of Science and Technology Agency.
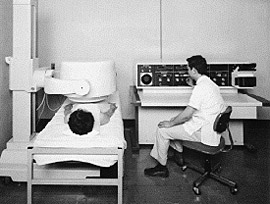
This camera was registered as a 25-cm gamma camera, type GCA-101 (photograph 1). It is the first Japanese camera for clinical use. It used a resistor matrix position computing circuit, which was the same type as that of N.C. Corp. Later, we developed and adopted the delay line type of position computing circuit under the joint research with National Institute of Radiological Sciences. We adopted a scintillator of 35 cm in diameter, 30 pieces of photomultiplier tubes, etc. Finally, we developed jumbo gamma camera, type GCA-202 (photograph 2).
 |
 |
Photograph 1
GCA-101 |
Photograph 2
35-cm gamma camera GCA-202 |
5. ICR and GCA-101 Gamma Camera
In the spring of 1969, the first gamma camera was delivered to Kohnodai Hospital. From then, we had many orders. In the fall of the same year, the 12th International Conference of Radiology (ICR) was held in Tokyo, where we displayed the GCA-101 gamma camera and the data processor.
The displays attracted much attention from foreign doctors and we received many inquiries. We started to export the cameras to Europe, which resulted in the establishment of Toshiba Medical Systems Europe B.V. We had to dispatch many service engineers to take care of after-sales service problems. It was a bitter experience.
In addition to Europe, the destination of exports covered the then Soviet Union, South America, Australia, etc. The new comers in charge of gamma camera had training courses in English conversation. Luckily or unluckily, many of them are now engaged in international business.
By the way, I happened to know, several years ago, that one of the camera had been sold to North Korea. The person in charge of sales at that time was assigned to the office in Europe, and he did not know it. I happened to be watching the TV news about the abduction. The news covered a hospital in North Korea and showed the controller panel of a medical device. It reminded me instantly of GCA-10l, because I had difficulty in designing the panel. At that time, some destinations of export were not known to us. After COCOM regulation started, the export to some countries was restricted. Around 1970, this camera was displayed at the exhibition held in Pyongyang, and sold in response to their request.
The GCA-101 displayed at Tokyo ICR is now preserved at Leiden University, the Netherlands. On the other hand, what has become of the camera that I happened to see in the TV news?
6. Subsequent Development of Gamma camera
After that, the writer left the work of the development of nuclear medicine equipment, and was assigned to the U.S. office in 1970. The writer's successor will describe the subsequent development of gamma camera (scinticamera), data processor, recorder, multi-recorder, SPECT and PET. Looking back on history, the writer feels that we succeeded in developing our unique technology, even though we imitated the overseas technology at the beginning. Many nuclear medicine engineers involved in that process later developed the CT technology, which was also unique and acceptable to the international market. This is probably the story of the good old days. |
