Nobuo Kumano(Former manager of Toshiba nuclear-medicine department) |
1. Introduction
-This is a sequel to " Development of Nuclear Medicine Equipment-1, by Shigeyasu Kurihara" in the previous issue-
In the previous issue, Mr. Kurihara described installation of the first Toshiba gammacamera at National Kohnodai Hospital (now, Kohnodai Hospital, National Center of Neurology and Psychiatry) in Ichikawa City, Chiba Prefecture.
I published two articles on the development of gammacamera at Tosiba(1), (2), where I mentioned mainly technical details and anonymized the persons concerned. As a result, the description lacked reality. In this article, I intend to write more vividly as far as I remember by referring to the documents remaining at hand.
I accessed the website, JIRA Virtual Museum, which listed historically and chronologically new products of several companies along with their catalogs, photographs and specifications. JIRA collected the de-classified information including other companies’ catalogs and specifications, which was not available to me while I was in office. The content of this website is very interesting.
However, there are also views that the content is formal and like captions on newspaper. It does not mention the stories behind the content, such as blatantly commercial deals and engineers' painstaking effort. From JIRA Virtual Museum, I excerpted the stories related to gammacamera and elaborated on them based on my experience in order to make this article more realistic.
But, my viewpoint may be unfair and biased because of my career as a Toshiba engineer. I should also apologize readers for my wrong memory or misunderstanding and missing information, if any.
2. The history of the gammacamera in Japan
The history of the nuclear medicine in Japan posted in JIRA Virtual Museum begins with the manufacture of a scintillation camera by Mr. Anger in 1956. He was an engineer in charge of production of experimental devices at University of California, Doner Laboratory. He registered the patent for the scintillation camera, the fruit of his ingenuity and experience in 1958, and granted exclusive licenses to Nuclear Chicago for commercial production. This was mentioned by Mr. Kurihara in the previous article.
In Japan, this patent motivated Mr. Mori, Aloka, to produce the first Japanese gammacamera and to announce it at the academic meeting. This product used nine Photo-Multipliers (hereafter PMs) of 50 mm in diameter and had the effective fields of view of 15 cm in diameter. While the camera was kept at The University of Tokyo Second Hospital, I asked Dr. Yasukochi to show it to me. I do not know what has become of that camera.
In 1967, Pho/GammaIII of Nuclear Chicago was imported via Marubun and Shimadzu and put into clinical use. Toshiba received the order of an Anger-type gammacamera from National Kohnodai Hospital under the condition of domestic production. We organized a development project team and delivered the first product to the hospital in 1969. This was also mentioned previously by Mr. Kurihara.
I was directly involved in the development task and experienced twists and turns in the process, which I detail here.
2.1. The birth of Toshiba gammacamera-- from functional prototype to commercial production
From 1962 to 1963, Toshiba experimented a camera using multistage image tubes, a kind of night vision equipment. But, it did not start development of an Anger-type scintillation camera. Judging from the general trend, we concluded that the Anger type was the best camera, and started immediately development aiming at commercial production. Six Nuclear Chicago cameras were imported to Japan. One of them was installed at The Cancer Institute Hospital, and I asked Dr. Onai to allow us to thoroughly investigate it. We met the radiological technologists there who used this camera and listened to them about operability of the camera. We attempted to understand the features, to add something new, and to produce a better product that supersedes it.
Technically speaking, the image was recorded as follows. Gamma rays, once detected, produce bright spots on a CRT screen with XY display. The spots form a latent image on an instant (Polaroid) film. Immediately after measurement, the film is developed to see an image formed by bright spots. If the spots are too bright, the image is white and blank. If they are too dark, nothing is seen. Thus, measurement must be carried out again. Anyway, a measuring instrument needs skill in operation.
We analyzed this survey information and designed a functional model. We divided the task of manufacturing of handmade parts and units among the development team members, and assembled them. We used a scintillator for detector that had been completed as Anger type for a functional prototype using multistage image tubes. We made a light guide that sends the light from the scintillator to PMs and disperses the light. We ingeniously made a matrix that amplifies the signal output of PMs through a preamplifier, and that performs position weighting. We used a commercial XY oscilloscope as a XY-CRT display for position signals. Thus, only in two months since development had been ordered, we completed a functional model to demonstrate principles ranging from a detector to a display. We moved a cobalt-57 point source of weak radioactivity in front of the detector. The flickering spots on the XY oscilloscope screen moved in synchronization with the movement of the radioactive source.
On the basis of this functional model, we designed a commercial product and delivered the first product to National Kohnodai Hospital in March 1969.
Unlike the above description, we actually encountered unexpected troubles in designing the product.
The schedule was tight, so we organized a project team and concentrated our efforts. The team leader was Mr. Kurihara. The team members included Mr. Katsurada (who entered the company one year ago) and the author (who entered the company four years ago) in charge of a detector and a position calculator, Mr. Asahina (who entered the company in the same year as I) for image display and Mr. Yuasa for mechanism design. All the members shared their design drawings on another and exchanged opinion for improvement. The completed drawings were transferred to the manufacture department for trial production.
We delivered successfully the first product, model GCA-101A, with 19 PMs of 76 mm in diameter and the effective filed of view of 25 cm in diameter. It was installed mainly by the engineers. However, it was not trouble-free. The units, which were acceptable in the functional prototype, did not work as expected. Even after installation, we continued experiments, found new defects, and retrofitted the camera with new parts. The hospital seemed to turn out to be our laboratory. We brought replacement parts to the hospital. We repaired the wirings of camera using a hand-held soldering iron and added the parts in order to meet the intended specifications. After reaching a certain level of satisfactory operation, we performed performance evaluation with Dr. Matsumoto and radiological technologists. We often stayed overnight for a week or so at the hospital to repeat adjustment from the very beginning. It took about two months for us to be given by Dr. Matsumoto the certificate of installation completion.
Incidentally, Toshiba decided to use the name of gammacamera henceforth instead of scintillation camera. Only Philips used the name of gammacamera. We wanted to differentiate our product by using a new name instead of conventional "scintillation camera" or "scinticamera". But, we did not register a trademark. We felt comfortable, however, to see the name of gammacamera gaining popularity.
2.2. Start of overseas sales strategy--from Australia to the Netherlands--
The International Conference of Radiology (ICR) was to be held in Tokyo in the fall of that year, October 1969. We were busy in improving the product design in preparation for that conference.
After ICR, Mr. Kurihara went to Australia for the sales campaign and contracted with Sydney Hospital at the center of Sydney City for the trial use of gammacamera. In January 1970, the author made his first overseas business trip for installation.
Despite the unexpected replacement of a detector during installation, I completed installation and orientation during the two-week stay. Thus, we began our overseas sales strategy in Australia. This camera was later transferred to a different hospital, because the performance was said to be inferior to that of Nuclear Chicago's camera. We faced severe international competition. Fortunately, the domestic sales increased. The second stage of export was Europe. In May 1971, we installed the first GCA-101A for the European market at Leiden University, the Netherlands.
2.3. Competition for higher intrinsic spatial resolution
According as the domestic sales increased, the preceding Nuclear Chicago was followed by other Japanese manufacturers such as Shimadzu and Hitachi Medico, resulting in severe competition in the market. The focus of competition was the higher intrinsic spatial resolution, which was measured by the minimum width of the lead slit placed in front of the detector. We continued to optimize those factors that influence the resolution in order to gradually improve them. The factors were the crystal of sodium iodide, light guide, PMs, preamplifier, position calculator and others. Some of the improvements were subcontracted. For instance, we visited a manufacturer of scintillator, Bicron in Ohio, the U.S. We discussed performance/quality control, the method to acquire more light from scintillator glass window, the best thickness of reflector around the crystal etc. We considered the importance of several factors, studied improvements and implemented them. We contacted a PMs manufacturer, Hamamatsu Photonics. We asked them to improve the quantum efficiency of a photoelectric surface in reference of RCA's PMs, which was a standard product at that time. We asked them to group PMs by sensitivity before assembly as a detector. Thus, we had a close relation with this company.

2.3.1. Resistor matrix type and delay line type
At that time, Dr. Tanaka, Director of Physics Division, National Institute of Radiological Sciences invented a position calculator to drastically improve the intrinsic spatial resolution of the Anger-type gammacamera. He started to develop this position calculator in 1969. This calculator used the delay line as the basic component and was called the delay line type. In order to apply this calculator to gammacamera, we offered a joint research for production of a prototype.
The conventional Anger-type resistor matrix type has the demerit in that the weighting is performed proportionately to the geometric location of PMs. When PMs are located far from the gamma-rays incidence point, larger weighting is performed despite the smaller amount of incident light from a scintillator. This increases the statistical noise in position calculation, increasing random noise, and decreasing accuracy of position calculation. On the other hand, the delay line type uses the delay line circuit to convert the PMs location into the time difference, and calculate the position. Weighting of position calculation is converted into the time. Moreover, when the time waveform is summed up by using a waveform shaping circuit, smaller weighting is given to the output signal of PMs located far from the incidence point. Thereby, the spatial resolution of a detector increased by 25% at a stretch. The product, model GCA-102A, was put into market in 1971.
Furthermore, the delay line type predicted the merit in that a larger effective field of view and more PMs than 19 do not decrease the special resolution, but contribute to enlarge the field of view. We used a larger detector with the field of view of 35 cm in diameter and 30 PMs for a jumbo gammacamera, Model GCA-202A, which was released in 1972. Industrialization of this model won The Mainichi Industry Award in 1973.
Hitachi Medico announced RC-1C-1205D claiming it as a new type in 1972, but it was actually a delay line type if I remember correctly.
2.3.2. Miniaturization of PMs
There was another way to improve the intrinsic resolution of detector. The gamma rays are absorbed by a scintillator and converted into photons. It was challenging how efficiently photons are led to the photoelectric surface of PMs to produce the position signals. The following is just like the Columbus's Egg. If you use more PMs with smaller diameter, you can improve relative resolution. This was demonstrated by model ON-100 of the U.S. Ohio Nuclear in 1973. They decreased the diameter of PMs from 76 mm to 50 mm, decreased the thickness of light guide, and improved the intrinsic resolution by about 30%. This was followed quickly by every manufacturer. Frankly speaking, Dr. Matsumoto, Kumamoto University often presented to us this idea of miniaturization, which we neglected without doing anything. When we knew Ohio's performance and technology, we were ashamed that we were less responsive as development engineers.
This improvement of resolution is disadvantageous in that that the number of expensive PMs increases, resulting in higher cost. For the 25-cm field of view, 37 PMs of 50 mm in diameter are needed instead of 19 PMs of 76 mm in diameter. For the 35-cm field of view, 61 PMs of 50 mm in diameter are needed instead of 30 PMs of 76 mm in diameter.
After making these improvements, Toshiba released a high-performance camera, model GCA-102S, of effective field of view of 25 cm in diameter and intrinsic resolution of 6.4-mm FWHM in 1974. Then, we announced an improved product, model GCA-401, of effective field of view of 35 cm in diameter and intrinsic resolution of 4.4-mm FWHM when the first World Conference of Nuclear Medicine was held in Tokyo in 1974, and released it in 1975. Hitachi Medico released a high-resolution gammacamera, model RC-1C-1635LD, with better intrinsic resolution of 3.6-mm FWHM in 1976, and won Kagaku Shimbun New Technology Development Award.
Thus, from 1968 through 1975, the intrinsic spatial resolution of the gammacamera was improved by leaps and bounds from 15-16 mm to 3.6 mm. After that, improvement stopped. Development continued for a square detector with large size or SPECT using detectors. The resolution of detector itself remained in 3.2-3.7 mm-FWHM. Naturally, the higher the intrinsic resolution of detector is, the better it is for clinical use. But, actually, a more dominant factor is the geometrical spatial resolution of the collimator itself on which the detector is mounted. The intrinsic resolution seemed to remain in this range. This situation is illustrated in Figure 1 Trend of intrinsic spatial resolution.
 |
Figure 1 Trend of intrinsic spatial resolution of gammacamera. |
2.4. Enlargement of effective field of view--From circular field with large diameter to square field
Toshiba released the gammacamera of the effective field of view of 35 cm in diameter ahead of other manufacturers in 1972. Then, the gammacamera of the effective field of view of 37 cm in diameter was released by the U.S. Nuclear Chicago as LFOV in 1975, and by the U.S. ON Inc. as Σ (sigma) 410 in 1976. In 1981, Technicare Inc. released their gammacamera, Ω (omega) 500, of the square effective field of view of 50 cm×35 cm. This camera made a strong impact on other manufactures by going against the common sense that the field of view should be circular. In line with this new trend, Toshiba also released model GCA-90A employing a square field of view in 1982. This camera was equipped with SPECT measurement function described later like Technicare's camera. Figure 2 shows the detector gantry and table of GCA-90A.
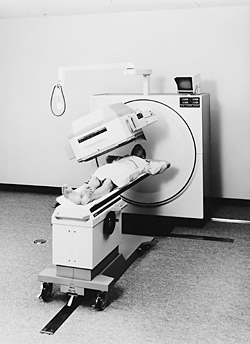 |
Fig. 2 Detector gantry and table of square jumbo gammacamera,
Toshiba GCA-90A
|
At the time of SPECT measurement, the detector of circular field of view produces the spherical region of measurement, whereas the square field of view produces the cylindrical region of measurement, which is advantageous to obtain wider range for SPECT measurement.
2.5. Development of cardiac, mobile, whole-body cameras--Difficulty of special-purpose cameras
According as the cardiac diagnosis is performed routinely with nuclear-medicine equipment, the special-purpose equipment was planned and developed for easy and simple clinical procedures.
For this purpose, the nuclide is limited to Technetium 99m or lower energy. The detector is light and small with the thin shield. The model GCA-10A was released as the dedicated camera for low energy in 1978. Its effective field of view is 25 cm in diameter. The collimator is light enough to be manually exchanged. This model developed into a mobile gammacamera, GCA-50A, which enables nuclear-medicine examination at the operating room, angiography room, and ICU/CCU, and was released in 1980. It is shown in Figure 3.
 |
Figure 3 Mobile gammacamera Toshiba GCA-50A
|
In Japan, however, the demand was lower than expected for RI administration and measurement in the general ward. Besides, Toshiba was four years behind Nuclear Chicago, which released the mobile Pho/Gamma/HP in 1976. For these reasons, the sales were not successful.
In 1974, Picker released Omni View, where the camera was stationary and the tabletop moved widthwise and longitudinally with a patient lying on the tabletop. This camera can perform whole-body measurement of bones and detection of tumors. Toshiba released the whole-body bed, GWA-101 in 1974 to be combined with gammacamera to enable whole-body measurement. For the initial detector of the effective field of view of 25 cm in diameter, 1.5 reciprocal movements (three strokes) were required for whole-body scans. Even for the field of view of 35 cm in diameter, one reciprocal movement (two strokes) was required. For the detector of square field of view of 50 cm×35 cm, however, only one stroke was required. In order to increase efficiency by scanning both front (AP) and back (PA) at the same time, we placed two square detectors facing oppositely each other. We developed the model GCA-90A-W2, the camera dedicated to whole-body scan in 1985, as shown in Figure 4.
 |
Fig. 4 Detector gantry and table of square 2-detector whole-body gammacamera,
Toshiba GCA-90A-W2 |
However, the cost performance was lower than expected, and the sales were not successful.
To be continued to the second half part (to be published in No. 64)
Bibliography
- History of nuclear medicine: JIRA Virtual Museum, http//www.jira-net.or.jp/vm/chronology_coremedi.html
- Shigeyasu Kurihara, Nobuo Kumano, Masamichi Katsurada, Eiji Kashio: The gammacamera and its peripheral equipment, Toshiba Review, 26, 2, 1971
- Nobuo Kumano: Latest nuclear-medicine diagnostic equipment, Toshiba Review, 34. 2, pp 108-113 (Showa 54-2) 1979
- Makoto Kakegawa et al.: Mobile gammacamera GCA-50A, Toshiba Review, 35, 10, pp 812-816, (Showa 55-9) 1980
- Nobuo Kumano: Nuclear-medicine diagnostic equipment, Toshiba Review, 38. 8, pp 691-695, (Showa 58-8),1983
- Nobuo Kumano: The radioisotope image by the gammacamera, Radioisotopes, 33, 12, 908-915, 1984
- Nobuo Kumano: Product information [II], Radiology Compendium, Vol. 36, In-vivo nuclear-medicine general remarks, 137-143, Nakayama Shoten (1985)
- Nobuo Kumano: 7. Gammacamera (1) SPECT-- The history from 1981 to 2000--, RADIOISOTOPES, 50, 96S-103S (2001)
- Nobuharu Yui: My history of nuclear medicine (2001)
- Nobuo Kumano: Lecture / "The relation of radiation and medicine" 6th session, Radiation and industry, No. 102, 64-71 (2004)
|
